
Fellowship
The Johns Hopkins University School of Medicine Medical and Public Health Laboratory Microbiology Fellowship Program is an American Society for Microbiology (ASM) postgraduate training program that is overseen by the Subcommittee on Postgraduate Educational Programs (CPEP).
CPEP is a 2-year fellowship program that prepares scientists and physicians for leadership roles in medical and public health microbiology laboratory careers.
Program Co-Director: Dr. Heba Mostafa, MD, PhD, D(ABMM), FIDSA
Program Co-Director: Dr. Andrew Clark, PhD, D(ABMM)
Case Spotlight
The Uninvited Guest: Bacterial spondylodiscitis
An elderly male presented with a three-month history of worsening lumbar pain. He endorsed a one-month history of chills and night sweats. While plain radiographs were unremarkable, an outpatient MRI revealed spondylodiscitis at L3-L4 with adjacent psoas abscess, prompting hospital admission. Computed tomography (CT) of the abdomen and pelvis revealed a right psoas abscess adjacent to the L3 inferior endplate, further suggesting an infectious process extending from the lumbar spine. The patient is originally from Central America, with recent travel to the continent within the last year. M. tuberculosis screening was negative.
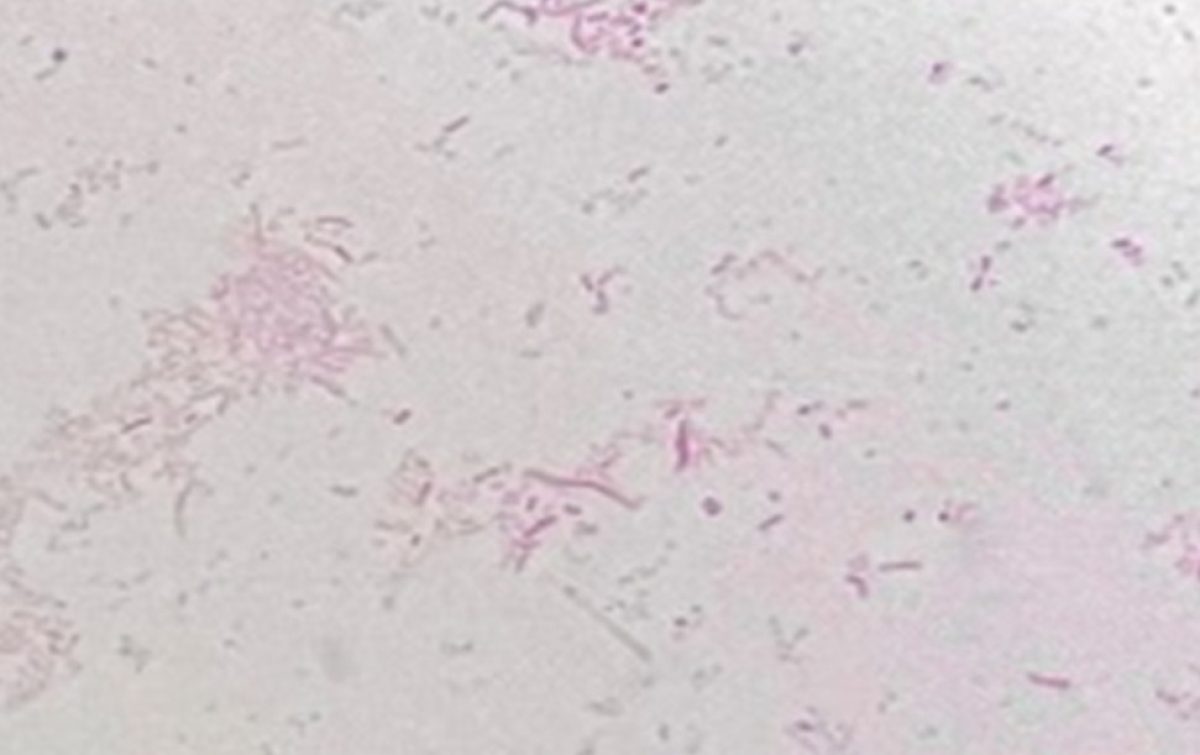
An IR-guided spinal aspiration of the accumulated serosanguinous fluid from the disc space yielded murky fluid which was sent for culture. Gram stain of the aspirate revealed moderate neutrophils, but no organisms were observed. Blood cultures were also obtained. Both blood and aspirate cultures turned positive after 48-72 hours of incubation and empiric therapy with ceftriaxone and vancomycin was initiated. Blood culture Gram stains and Gram stains from the punctate colonies recovered from the aspirate revealed small Gram-negative coccobacilli. Importantly, growth was observed on Sheep blood agar (BAP) and chocolate agar, but growth was noticeably absent from the MacConkey agar suggestive of a fastidious organism. Biochemical testing revealed positive oxidase, catalase, urease, and β-lactamase results. Due to a concern for a possible laboratory biological hazard, further manipulation of cultures containing suspect organisms were performed using enhanced biosafety precautions
MALDI-TOF mass spectrometry was performed for identification without success using FDA-cleared and RUO databases. Per laboratory protocol, a Security Relevant database for the identification of Select Agents was attempted, identifying this organism as Brucella sp. The isolate was subsequently referred to the Maryland Department of Health (MDH) laboratory, which confirmed as B. abortus by a Brucella-specific PCR assay. Antimicrobial therapy was adjusted to a combination of PO doxycycline and rifampin to be continued for three months. Following initiation of appropriate therapy, the patient’s symptoms significantly improved and they were discharged after one week of hospitalization.
Which of the following is/are false?
A. Brucella species are classified as BSL-3 organisms, requiring strict biosafety precautions.
B. Brucella species are fastidious and require X or V factors or both for growth.
C. Gram stain may appear faint because the organisms are small intracellular coccobacilli.
D. Brucella species exhibit positive results for oxidase, catalase, and urease tests.
Bilateral Ocular Symptoms in a Cat-Exposed Host
A middle-aged adult with a history of alcohol and tobacco use disorder, underlying COPD, progressive weight loss with cachexia presented with a one-month history of worsening bilateral eye pain, photophobia, excessive tearing, and decreased vision. The patient lives with domestic partner and three domestic cats. There was no reported history of ocular trauma.
At the time of presentation, the patient was near blindness with markedly decreased visual acuity in both eyes. There was severe blepharitis with meibomian gland dysfunction bilaterally. Slit-lamp examination demonstrated inferior limbal corneal opacity and stromal thinning (right greater than left), bilateral layering hypopyon, and posterior synechiae of the iris. The overall presentation was concerning for bilateral hypopyon anterior uveitis with corneal thinning. Given the atypical bilateral involvement, both infectious and autoimmune etiologies were considered.
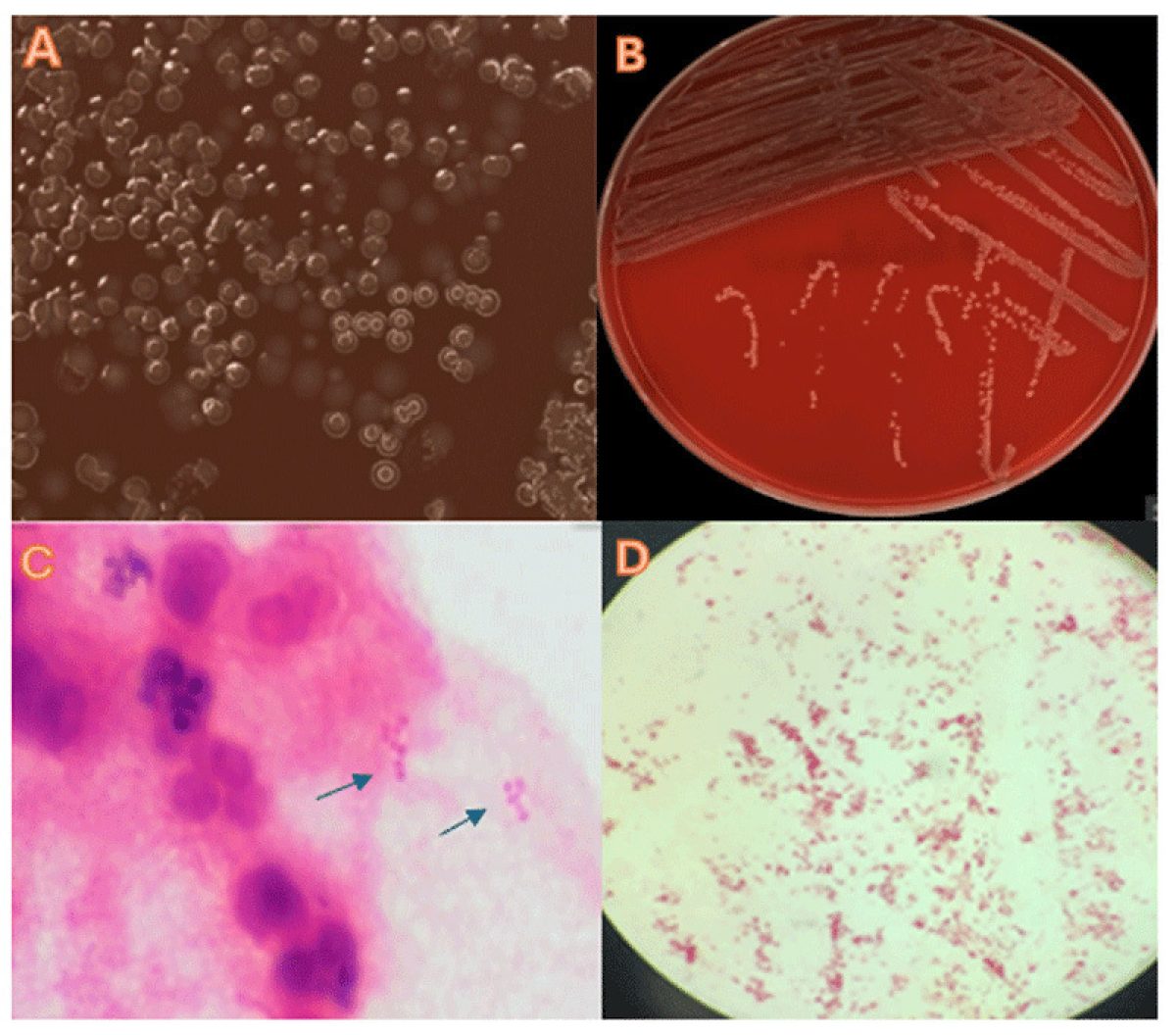
Corneal cultures were obtained prior to antimicrobial escalation. Empiric topical moxifloxacin was initiated along with erythromycin ophthalmic ointment. Doxycycline and valacyclovir were also started while awaiting microbiologic data and serologic workup. Gram stain from the corneal scraping demonstrated numerous polymorphonuclear leukocytes and small Gram-negative rods. Culture on 5% sheep’s blood agar and chocolate agars demonstrated heavy growth of a gray, nonhemolytic organism within 24 hours. Importantly, no growth was recovered on MacConkey agar. The predominant recovered organism was oxidase-, catalase-, and indole positive.
Question 1
Based on microbiologic findings and biochemical reactivity, which organism is the most likely primary pathogen?
A. Haemophilus influenzae
B. Neisseria gonorrhoeae
C. Pasteurella multocida
D. Pseudomonas aeruginosa
E. Eschrichia coli
Question 2
Which epidemiologic detail in this case most strongly supports the likely source of infection?
A. Chronic tobacco use
B. Underlying COPD
C. Chronic alcohol use disorder
D. Living with three domestic cats
E. Bilateral eye involvement
What a pain in the neck! - An Infected Branchial Cleft Cyst
A young male with a history of a recurrent left branchial cleft cyst presented to the Pediatric Emergency Department with a two-day history of worsening left-sided facial swelling. The cyst was first identified five months prior to the current encounter as a left submandibular abscess seen on CT. He underwent bedside incision and drainage concomitantly receiving an inpatient course of IV ampicillin/sulbactam and trimethoprim/sulfamethoxazole. He was ultimately discharged home on PO amoxicillin/clavulanate. The cyst decreased in size but was never fully resolved, then gradually enlarged over the next month, and became painful to the touch. A computed tomography (CT) scan was scheduled for visualization, but a day before the imaging appointment it was noted the cyst doubled in size, resulting in the patient presenting to clinic.
The CT revealed a fluid-filled collection (approximately 3 x 2 x 3 cm) consistent with previous imaging. The patient was afebrile despite an elevated white blood cell count, and no erythema or fluctuance was observed. A second incision and drainage was performed yielding 3mL of purulent material which was submitted to the clinical microbiology laboratory for culture. The patient’s symptoms improved following the procedure, and he was admitted to pediatrics for monitoring. He received IV ampicillin/sulbactam, ultimately transitioned to PO amoxicillin/clavulanate at discharge.
Gram stain of purulent samples showed heavy polymorphonuclear leukocytes and heavy Gram-negative bacilli. After one day, culture yielded heavy, pure growth on chocolate agar with grey colonies. Organisms in the culture were definitively identified by MALDITOF‑TOF as Neisseria lactamica.
Which of the following review questions about Neisseria lactamica is false?
A. Neisseria lactamica is a common commensal organism found in the nasopharynx of children.
B. Neisseria lactamica is oxidase and catalase positive and ferments glucose and lactose.
C. Neisseria lactamica in the pharynx increases the likelihood of Neisseria meningitidis colonization.
D. Transmission of Neisseria lactamica mainly occurs through respiratory droplets.
Testicular pain in an adult
The patient is an adult who immigrated from Central America many years ago with no past medical history who presents to the emergency department complaining of right testicle pain and swelling. The pain began about 4 days prior to presentation and was mild at first but became severe 24 hours prior to presentation. The patient denied nausea, vomiting, diarrhea, abdominal pain, or genital lesions, but endorsed one episode of dysuria. They reported that two weeks prior, they had cough and rhinorrhea followed by subjective fevers, intermittent headaches, and cervical lymphadenopathy. The patient has no history of sexually transmitted infection and is sexually active with one partner. An ultrasound exam with doppler of the testicle revealed normal blood flow.
Which of the following is NOT accurate about this patient’s condition?
A. The presentation is caused by a reportable infection.
B. Emergent orchiopexy is required.
C. The infection is preventable with a live-attenuated vaccine.
D. Sialic acid plays an important role in pathogenesis.
Hematuria and Leg Pain in an Adolescent With Influenza
An early adolescent presented during the 2025–2026 influenza season with hematuria and bilateral leg pain. The patient had no underlying medical conditions, no history of trauma, and did not participate in sports or regular exercise. The leg pain was described as severe, aching pain extending from the thighs to the calves, without associated tingling or numbness, and was significant enough to impair ambulation. There was no urinary frequency, urgency, dysuria, discharge, or flank pain. Symptoms developed after several days of a mild upper respiratory tract infection. The patient tested positive for influenza A and had markedly elevated creatine kinase levels. The overall diagnosis was nontraumatic rhabdomyolysis, most likely secondary to influenza A infection.
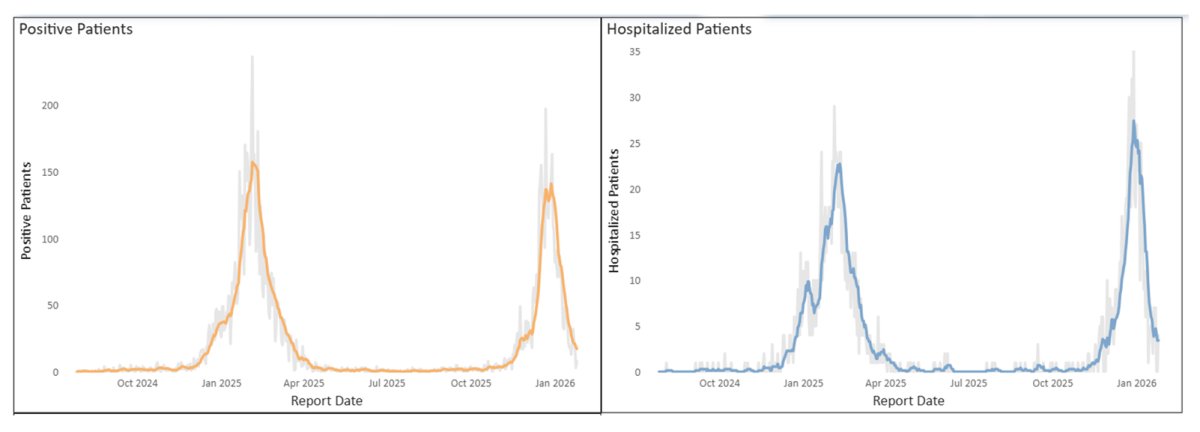
The 2025- 2026 Influenza Season Update
The 2025–2026 influenza season was characterized by earlier epidemic activity in the Northern Hemisphere and the global emergence of influenza A(H3N2) subclade J.2.4.1 (H3N2 subclade K). At the Johns Hopkins Health System (JHHS), influenza activity increased beginning in November 2025, approximately one month earlier than during the previous season. Peak test positivity occurred in late December 2025, in contrast to an early February peak in the 2024–2025 season.
Influenza A virus
Influenza A is one of the primary types of influenza viruses that infect humans and is classified into subtypes based on the surface glycoproteins hemagglutinin (H) and neuraminidase (N) (1). Influenza A viruses are associated with great genetic diversity through antigenic shift and drift. Transmission occurs primarily through respiratory droplets and aerosols generated by infected individuals, as well as through contact with contaminated surfaces (2). Common clinical manifestations include fever and chills, cough, sore throat, myalgias, headache, and fatigue; gastrointestinal symptoms such as vomiting and diarrhea may occur, particularly in pediatric patients (3). Annual influenza vaccination remains the most effective measure for reducing disease severity.
Increased numbers of cases, increased likelihood of rare complications
With increased numbers of influenza infections, complications, including rare extrapulmonary manifestations, are increasingly recognized. Influenza A–associated rhabdomyolysis is an uncommon but potentially severe complication that can lead to acute kidney injury and renal failure (4, 5). Rhabdomyolysis is characterized by skeletal muscle breakdown, resulting in the release of intracellular contents that can cause renal injury. It may arise from traumatic muscle injury or from non-traumatic causes, including ischemia, hyperthermia, infections, or medication exposure. Among infectious etiologies, influenza A has been identified as a more common trigger of rhabdomyolysis compared with SARS-CoV-2, HIV, and coxsackievirus (6). Creatine kinase (CK) levels exceeding 1,000 U/L are commonly used to support the diagnosis of rhabdomyolysis. Notably, during the 2009 H1N1 influenza outbreak, a report showed that 62% of patients with influenza A associated pneumonia were reported to have elevated CK levels (7).
Case by: Alona Malacas and Heba H. Mostafa
References
1. Kim H, Webster RG, Webby RJ. 2018. Influenza Virus: Dealing with a Drifting and Shifting Pathogen. Viral Immunol 31:174-183.
2. Killingley B, Nguyen-Van-Tam J. 2013. Routes of influenza transmission. Influenza Other Respir Viruses 7 Suppl 2:42-51.
3. Anonymous. https://www.cdc.gov/flu/hcp/clinical-signs/index.html.
4. Nanduri RS, Karnath N, Gurram A, Ali A, Karnath B.2025. Rhabdomyolysis secondary to Influenza A infection in a patient using antipsychotic and serotonergic agents: A case report. SAGE Open Med Case Rep 13:2050313x251392105.
5. Agarwal A, Kaplan J, Bahoora J, Keirn R. 2020. A Case of Influenza A-induced Rhabdomyolysis Resulting in Hemodialysis Dependent Renal Failure. Chest 158:A468.
6. Anonymous. https://www.omicsonline.org/peer-reviewed/rhabdomyolysis-in-the-context-of-infections-combining-the-elements-135294.html.
7. Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Quiñones-Falconi F, Bautista E, Ramirez-Venegas A, Rojas-Serrano J, Ormsby Christopher E, Corrales A, Higuera A, Mondragon E, Cordova-Villalobos Jose A.Pneumonia and Respiratory Failure from Swine-Origin Influenza A (H1N1) in Mexico. New England Journal of Medicine 361:680-689.
Post-Laceration Cellulitis After River Water Exposure
A teenage male presented to the ED with a 3 cm horizontal laceration over the left patella. The injury occurred while he was playing in a shallow river at a state park and the patient tripped over a rock. The wound was initially contaminated with river water, mud and sand. Upon presentation, his caregiver irrigated the wound with saline, and he received four sutures to ensure closure of the laceration. He was discharged on oral cephalexin (500mg for 7 days). The following day, he returned to the ED with worsening knee pain, swelling, and inability to flex the joint. He was hypertensive, and laboratory tests revealed an elevated CRP (11 mg/L) but normal WBC counts. The wound was now exhibiting mucopurulent drainage and erythema consistent with cellulitis, so the patient was admitted to the general pediatrics service for management.
After hospital admission, the wound was incised and drained and the purulent drainage material was sent to the microbiology laboratory for culture. The patient was started on IV clindamycin and cefepime to expand antibiotic coverage. No imaging was performed to assess deeper infection or joint involvement. The patient reported significant improvement following the drainage procedure. A day later, the culture revealed moderate growth a beta-hemolytic, Gram-negative organism which was definitively identified Aeromonas spp. in addition to a mixture of skin and enteric flora.
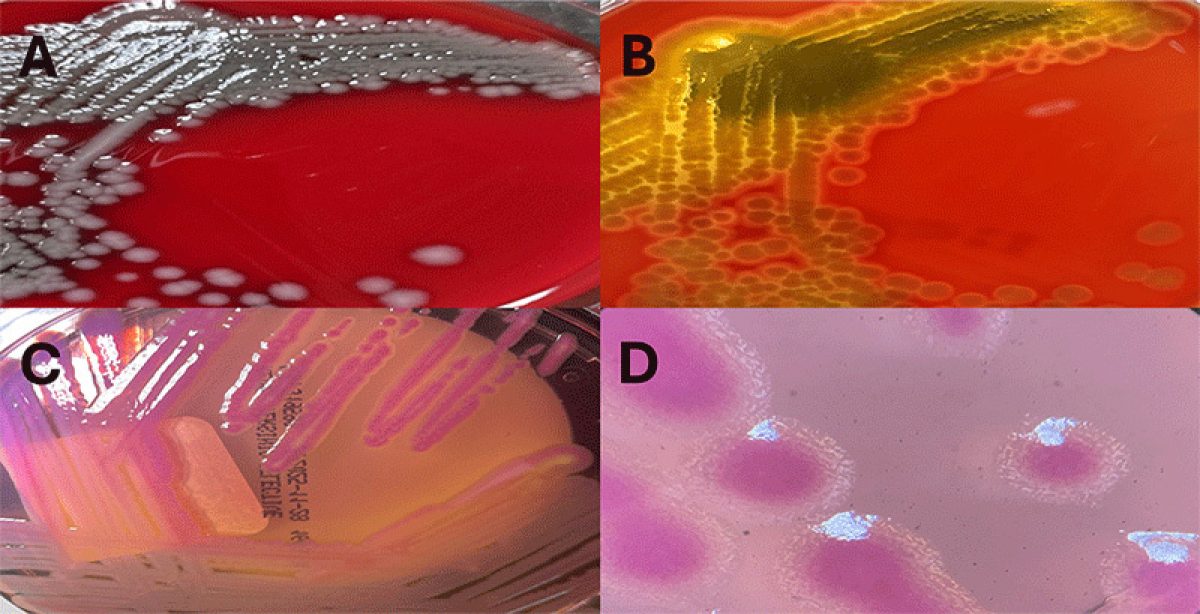
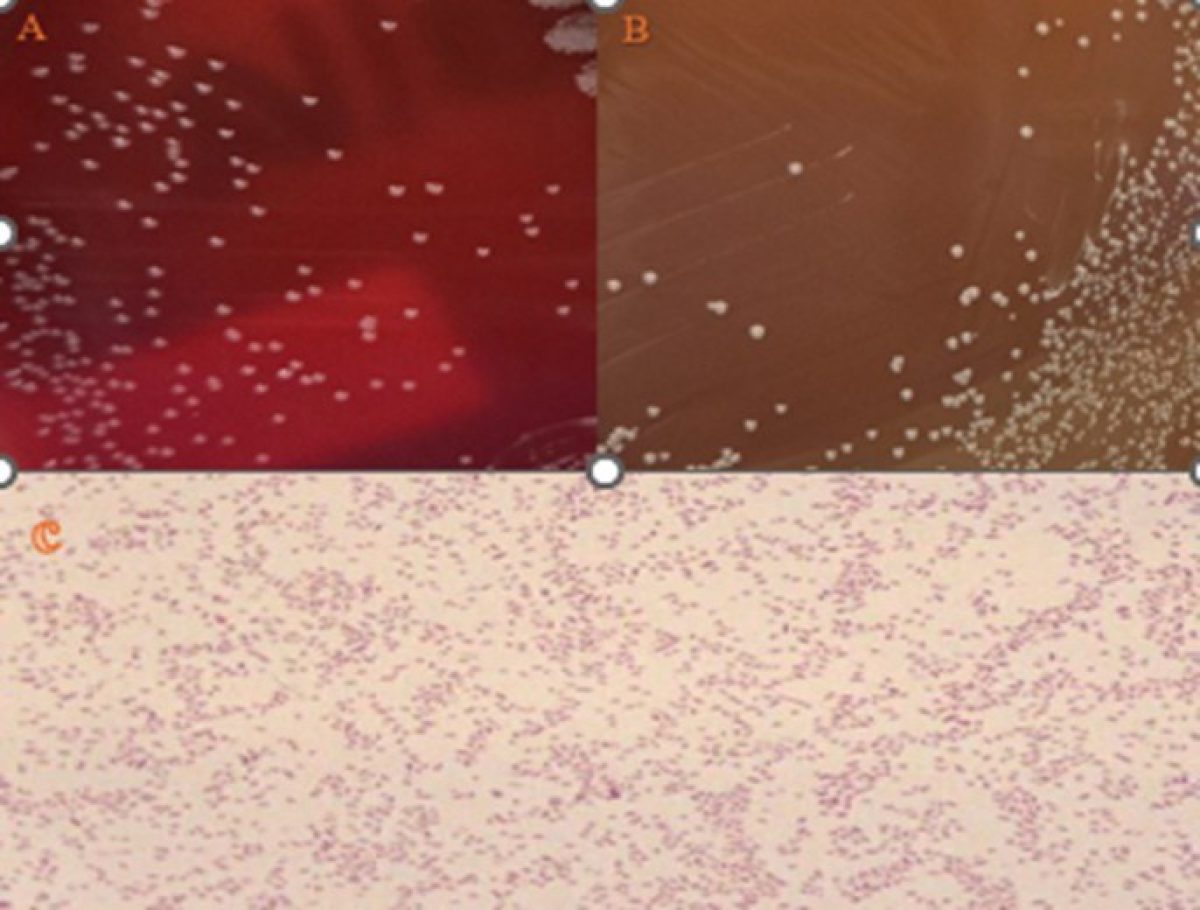
Representative images of Aeromonas spp. in culture on blood agar and CIN media.
A) Colony morphology on blood agar. B) Characteristic beta-hemolysis on blood agar.
C) Characteristic growth on CIN media. D) “Bull’s-eye” colony morphology on CIN media.
Which of the following review questions about Aeromonas spp. are false?
A. Aeromonas spp. primarily inhabit aquatic environments, including both fresh- and brackish water ecosystems.
B. Aeromonas spp. infections occur most frequently during warmer months, typically from May to October.
C. Aeromonas spp. mainly cause two types of infections: gastroenteritis and wound infections, sometimes accompanied by bacteremia.
D. Aeromonas spp. yield negative results for both oxidase and indole tests.
Persistent Fevers After Lyme Treatment
A 74-year-old male with a history of Hodgkin's lymphoma presents with recurrent fever, fatigue, and night sweats. He was evaluated 10 days ago for similar symptoms and diagnosed with Lyme disease, for which he received IV ceftriaxone. During a recent heat wave, he experienced sudden fatigue, energy loss, tremors, and night sweats. Although the night sweats have subsided, he continues to have chills and intermittent fevers, with a recent spike to 104°F. He reports muscle and joint aches and has increased his fluid intake using Gatorade and Liquid I.V. to prevent dehydration. The COVID-19 test is negative. No cough, shortness of breath, or other respiratory symptoms are present. No weight loss, changes in taste or new rash have been noted. He has spent significant time outdoors over the past month.
Laboratory workup revealed findings suggestive of hemolysis including increased LDH and increased white blood cells count with a neutrophil predominance. Malaria smear by giemsa-stained thin and thick smear is positive for Babesia and % Parasitemia = 1.7%.

Which of the following is false regarding Babesiosis?
A. Symptoms of Babesiosis typically begin 1 to 4 weeks after exposure to the parasite
B. Babesiosis is transmitted through tick bites or blood transfusion
C. Co-infection with Lyme disease is possible
D. Babesia microti is a rare cause of symptomatic Babesiosis in the U.S.
A Day at the Bench… In a Few Minutes
Babesia
Listeria Monocytogenes
Mycobacterium Tuberculosis
Geotrichum
Hepatitis C Virus
Malaria
Pipetting
Streaking Plates
Podcast
Dive into the fascinating world of microorganisms with our curated selection of podcasts on microbiology.
Learn About Microbiology
Explore careers, training opportunities, and hands-on experiences in microbiology. Whether you're a student, trainee, or professional, you can learn about the field, connect with our lab, and apply for educational programs.
Explore Microbiology Careers
- Learn what microbiologists do and the different lab career paths available
- Discover training and certification options, including the CPEP Fellowship
Visit or Shadow Our Lab
- Request a lab tour: Pathology Laboratory Tour Request Form
- Shadow for the day: Pathology Laboratory Shadow Request Form
Training and Educational Programs
Apply for short-term opportunities:
- Observership (through Johns Hopkins Medicine)
Requires prior approval from the Education Coordinator and/or Division Director - Visiting Medical Student Program
View program details and application information - Elective Rotation for Pathology Residents
(note: This requires initial approval from the Education Coordinator and/or Division Director) Contact Dr. Heba Mostafa ([email protected]) - Visiting Scientist Program
Requires approval from the Education Coordinator and/or Division Director
Contact: Dr. Heba Mostafa ([email protected]) - Industry Training
Contact: Dr. Heba Mostafa ([email protected])
Contact the Microbiology Lab
For questions or additional information: [email protected]