
Pain Assessment
The first step in pain management is a thorough assessment. Your healthcare provider will want to know many details about the pain. When did it start? How often does it occur? Where is it located? What does it feel like? Is it stabbing, shooting, dull, cramping or aching? How intense is it on a scale of 0 to 10? What things make it better or worse? What medications or other treatments have been used, and how well have they worked? Have these treatments had significant side effects? It's also important to consider the effect that the pain is having on your own life and the lives of your family members and significant others.
Pancreas Cancer and Pain Management by Dr. Michael Erdek
Treatments
The main way that pain from pancreatic cancer is treated is with opioids (or narcotics). These are the strongest pain relievers available and are only available by prescription. Other non-opioid medications include Acetaminophen (or Tylenol) and nonsteroidal anti-inflammatory drugs (or NSAIDs).
The most commonly used opioids for treatment of the pain caused by pancreatic cancer are morphine, oxycodone, Dilaudid, or fentanyl. Non-opioids which are available over-the-counter and are frequently used include Tylenol, ibuprofen, Motrin, Advil and Aleve. In addition to oral medications, skin patches may be used. This forms a strong foundation of pain control.
Episodes of pain between doses is of pain medication is referred to as breakthrough pain. A short-acting, immediate release opioid is usually prescribed for breakthrough pain. If these short-acting medications are inadequate, then you may be prescribed a long-acting opioid, which may last 12, 24, or even 72 hours.
It's important to note that many pain medications have side effects. Common side effects include sedation, nausea, itching or constipation, and a stool softener is recommended for all patients using opioid medications.
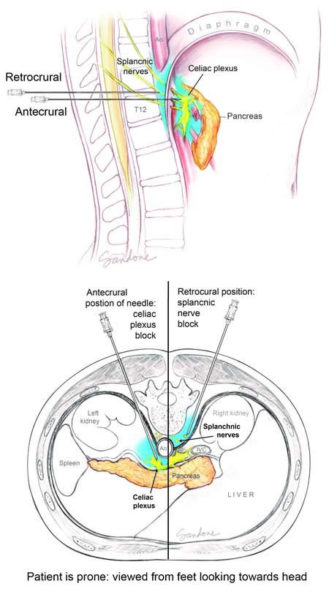
Celiac Plexus Block
For patients who do not respond to these medications or who have unacceptable side effects, a celiac plexus nerve block may be performed. In this procedure, anesthesia is injected close to a group of nerves, situated in the back of the abdomen, that carry pain signals from the pancreas to the brain. This is done under x-ray guidance with the patient lying face down. Local anesthetic is used before placement of the celiac plexus block needles, and the patient is comfortably sedated. The needles are placed and a small amount of local anesthetic is delivered to the area of the nerves in the back of the abdomen. If pain relief is appreciated, then strong alcohol is injected through the needles to create a long-lasting block of these nerves.
The nerve block may last up to three or four months, although the block tends to wear off over time. Blocks can be repeated if necessary. This nerve block can be performed in an outpatient setting, or at the time of surgery.
Celiac Plexus Block for Pancreatic Cancer Pain
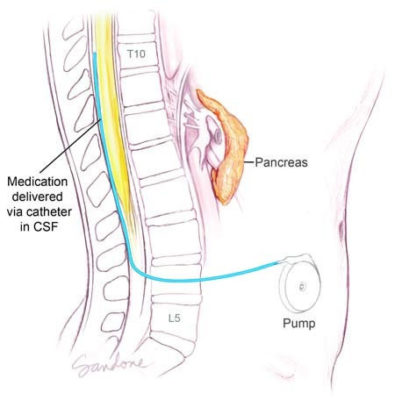
Epidural and Intrathecal
Patients who still have pain which cannot be controlled with oral medications or nerve block procedures may require epidural or intrathecal anesthesia. A small catheter is placed into the spine to deliver pain medication directly into the spinal fluid, similar to what is done for women in labor and delivery. The catheter is usually placed on a temporary basis for a few days with the patient in the hospital, and if it's successful, the patient can have a more permanent pump and catheter implanted under the skin. This surgery is done under general anesthesia, and the patient is admitted overnight to the hospital and sent home the next day.
The pump can be refilled with medication by your doctor on average between every one to three months. This method can be very effective, but requires special physician and nursing expertise and needs careful monitoring.
Intrathecal Pump for Pancreatic Cancer Pain Management