
A diagnosis of pancreatic cancer is frightening and confusing. It's hard to know where to start with finding treatment.
The primary determinant of how a patient should be treated is the stage of the tumor, as stage determines if a tumor can or cannot be removed (resected) surgically. Small, locally confined tumors are best treated with surgery. Large cancers that have spread to other organs are best treated with chemotherapy. While this may sound simple, the treatment of patients with pancreatic cancer is often complex, and the best treatment is sometimes unclear. For example, some cancers are in between localized and metastatic. "Locally advanced" cancers are intermediate-sized cancers that haven't spread to other organs but have invaded nearby (local) structures. We have established a multi-disciplinary clinic to evaluate locally advanced and other complex cases.
The best way for a patient to determine where to start is to answer the questions below. If you are still uncertain, then simply call 410-933-PANC (410-933-7262) to make an appointment.
Can the Tumor Be Removed With Surgery?
The best way to answer this question is to answer the four questions in the drop-downs below. If, in answering these four questions, you believe the tumor is removable ("operable"), we advise you to make an appointment with one of our skilled surgeons.
If the tumor cannot be removed, skip the four drop-downs and proceed to the "when the tumor cannot be removed" section.
What is the location of the pancreas cancer? ▼
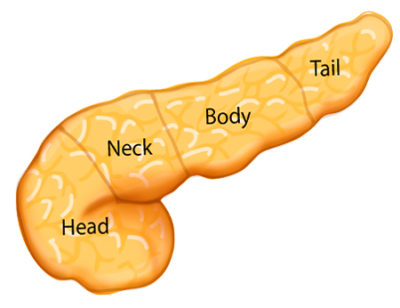
The location of the pancreas cancer, as visualized by CT scan, will determine the type of the operation.
Cancers of the head of the pancreas may be surgically removable with a pancreaticoduodenectomy or Whipple operation.
Cancers of the body or tail of the pancreas may be surgically removable with a distal pancreatectomy. In removing the body and tail of the pancreas, we often also remove the spleen, because of the very close contact of the two organs, and to better remove the lymph nodes between the two organs. In selected cases tumors in the body or tail of the pancreas may be removed using minimally invasive approaches such as robotic and laparoscopic pancreatectomy.
Is the cancer growing into a major blood vessel? ▼

Typically high definition three-dimensional CT scanning is used to determine whether the cancer is growing into any of the major blood vessels that pass right next to the pancreas. At Johns Hopkins we use cutting-edge 64 or 32 detector CT machines as they provide significantly better quality images.
Specifically, the major blood vessels we examine are the portal vein/superior mesenteric vein (drains blood from the intestines to the liver), superior mesenteric artery (supplies blood from the heart to the intestines), and the hepatic artery (supplies blood from the heart to the liver).
If the cancer only partially involves these vessels, a combination of radiation and chemotherapy may be used to shrink the tumor so that it becomes small enough to be removed surgically. We call this down staging of the cancer.
If there is extensive involvement of these major blood vessels, the pancreas cancer may never become surgically removable even with treatment. These are unresectable because of the local extent of the disease. In these instances the cancer is best treated medically, or with a combination of chemotherapy and radiation therapy.
Has the pancreas cancer already spread? ▼
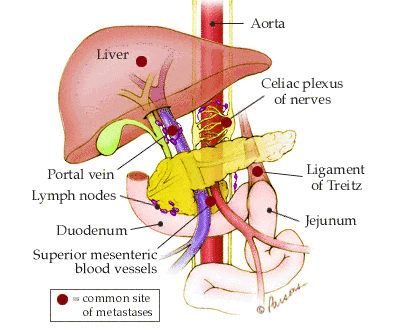
We often determine whether the pancreas cancer has spread (metastasized) to other organs/areas by looking at the CT scan. The organs/areas that we sometimes see evidence of spread are the surrounding lymph nodes, liver, abdominal cavity, and lungs. These areas show up as suspicious abnormal spots that we do not normally see in those locations. If there is evidence of disease spread to the lymph nodes immediately adjacent to the pancreas, many times the disease can still be surgically removed. This is because lymph nodes around the pancreas are removed with the pancreas at the time of surgery.
However, if there is evidence of disease spread to the liver, abdominal cavity, and or lungs, then the disease is not surgically removable (we call these unresectable).
Sometimes we order a PET/CT scan to help clarify whether there is evidence of metastasis. This test measures how much sugar each area of the body is using and tries to determine the likelihood of there being cancer in that location. If metastases are identified, the pancreas cancer may not be surgically removable (unresectable). In these instances the cancer is best treated medically.
Will the patient be able to tolerate an operation? ▼
The decision of whether a patient will be able to tolerate an operation is very complex and best made by a very experienced team. Studies show that patient outcome is best at high volume surgical centers. Surgeons at Johns Hopkins have performed over 5,000 Whipple resections, more than any other institution in the world. Age by itself does not exclude anyone from an operation. We have successfully performed a Whipple operation on a patient over 100 years old. More important than age is the condition of the patient's body and how well their major organs are functioning. If the disease is determined to be resectable, the next step is to schedule surgery.

When the Tumor Cannot Be Removed
Locally advanced cancers:
If your pancreatic cancer grows beyond the confines of the pancreas and invades surrounding vital structures it may be considered "locally advanced" by your surgeon. A pancreatic cancer in the head of the pancreas is locally advanced when the tumor has invaded the superior mesenteric artery or the superior mesenteric vein (two large blood vessels that pass next to the pancreas). Pancreatic cancer in the body and tail of the pancreas is locally advanced when the tumor has invaded the blood vessels called the celiac artery and the hepatic artery.
The determination of locally advanced pancreatic cancer is based on a careful evaluation of a high quality, detailed, thin section
three-dimensional CT scan of the pancreas sometimes with supporting information from an endoscopic ultrasound or ERCP. The determination of whether a pancreatic tumor is locally advanced should be made by an experienced pancreatic surgeon since in selected situations locally advanced tumors may be resectable by an experienced pancreatic surgeon with specialized techniques including localized resection of the blood vessels. In some cases chemotherapy and/or radiation can be used to shrink locally advanced tumors so that they can become resectable.
If after careful evaluation, a locally advanced pancreatic tumor is not thought to be resectable, then chemotherapy and radiation therapy can be used to slow down growth of the tumor and decrease the pressure of the tumor on surrounding structures in the hope of improving symptoms.
Metastatic cancers:
Cancers that have spread to other organs, such as the liver, are called metastatic cancers. They usually cannot be removed surgically. Instead, patients with metastatic (stage 4) pancreatic cancer are almost always treated with chemotherapy by an expert oncologist.

I am not sure if my tumor can be removed
Often patients and doctors who do not routinely take care of patients with pancreas cancer are not sure as to whether a pancreas cancer is surgically removable or not. That determination can be difficult, especially when a cancer is locally advanced. It is very important that patients have good imaging studies, and, when there is any question, that their case is discussed in a multidisciplinary pancreas cancer conference in which there are many doctors from different specialties present (surgeons, medical oncologists, radiation oncologists, pathologists, gastroenterologists, radiologists, etc.)
I have a Cyst or an IPMN
Not all masses in the pancreas are cancer. Cysts, including intraductal papillary mucinous neoplasms, are surprisingly common. The team at Johns Hopkins has extensive experience managing patients with cysts and IPMNs.
I have a Neuroendocrine Tumor
Although neuroendocrine tumors are rare, they are important to recognize because their treatment is completely different from most other tumors of the pancreas.