Invasive pancreatic cancer starts from well-defined precancerous lesions. These precancerous lesions are subdivided into two types. The small lesions are called "pancreatic intraepitheliel neoplasia (PanIN)," and the larger lesions are called intraductal papillary mucinous neoplasms (IPMNs). This section will focus on PanIN lesions. IPMNs are discussed elsewhere on this site.
Classification of Duct Lesions in the Pancreas
The history of how precancerous duct lesions were recognized and studied is of interest. While the lesions have been recognized for more than a century, the real breakthrough in naming these lesions came in 1999. In September 1999, a Pancreas Cancer Think Tank sponsored by the National Cancer Institute was held in Park City, Utah. Several workshops were held at this Think Tank, including a pathology workshop focusing on the nomenclature of duct lesions in pancreas. The duct lesions discussed were those that involve the smaller caliber ducts. They do not involve the main pancreatic duct, and they generally are too small to be seen grossly or by radiologic imaging. Participants in the meeting agreed to establish the first formal nomenclature and diagnostic criteria for precancerous duct lesions. This nomenclature was revised in 2014 at a think tank held at Johns Hopkins.
Categories of Duct Lesions
Below are the categories of the duct lesions:
Normal
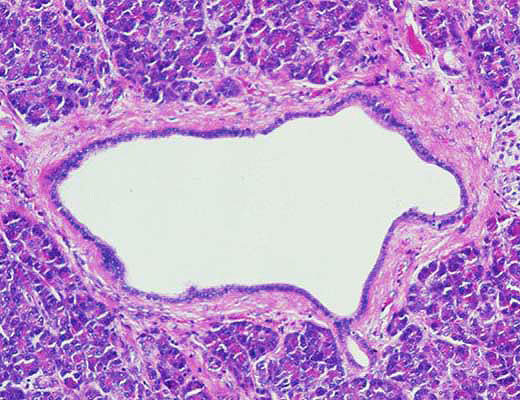
The normal ductal and ductular epithelium is a cuboidal to low-columnar epithelium with amphophilic cytoplasm. Mucinous cytoplasm, nuclear crowding and atypia are not seen.
Squamous (transitional) Metaplasia
A process in which the normal cuboidal ductal epithelium is replaced by mature squamous or transitional epithelium without atypia.
Low-grade
Low-grade pancreatic intraepithelial neoplasia encompasses three older terms- PanIN-1A, PanIN-1B and PanIN-2.
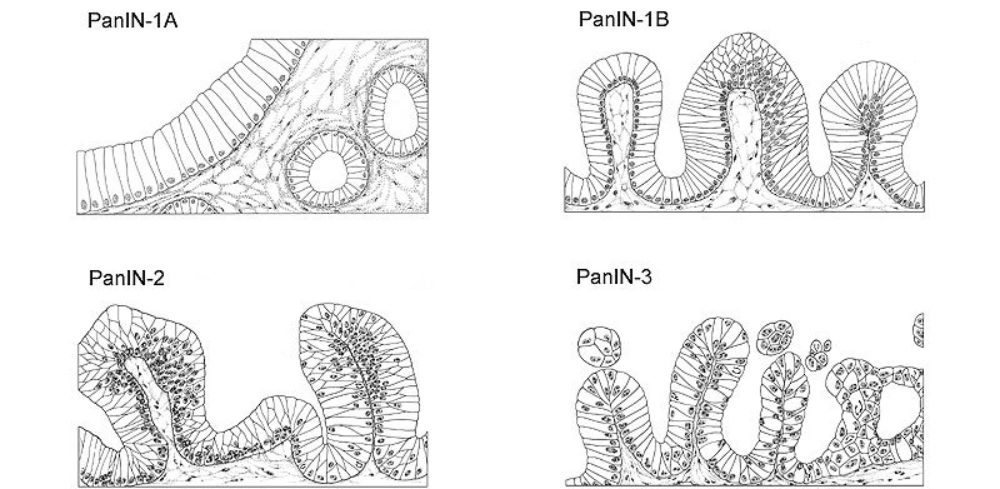
PanIN-1A: (Pancreatic Intraepithelial Neoplasia 1-A): These are flat epithelial lesions composed of tall columnar cells with basally located nuclei and abundant supranuclear mucin. The nuclei are small and round to oval in shape. When oval the nuclei are oriented perpendicular to the basement membrane. It is recognized that there is considerable histologic overlap between non-neoplastic flat hyperplastic lesions and flat neoplastic lesions without atypia. Therefore, some may choose to designate these lesions with the modifier lesion ("PanIN/[L]-1A") to reflect the fact that the neoplastic nature of many cases of PanIn-1A has not been established.
PanIN-1B: (Pancreatic Intraepithelial Neoplasia 1-B): These epithelial lesions have a papillary, micropapillary or basally pseudostratified architecture, but are otherwise identical to PanIN-1A.
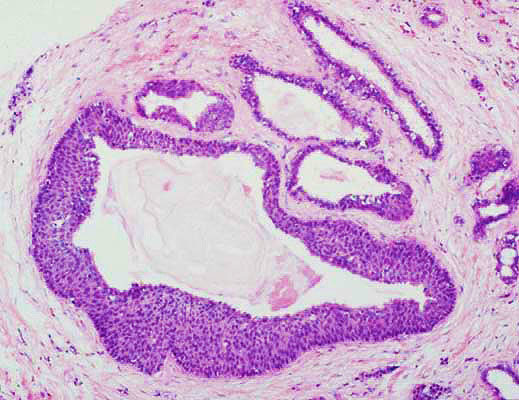
PanIN-2: (Pancreatic Intraepithelial Neoplasia 2): Architecturally these mucinous epithelial lesions may be flat or papillary. Cytologically, by definition, these lesions must have some nuclear abnormalities. These abnormalities may include some loss of polarity, nuclear crowding, enlarged nuclei, pseudo-stratification and hyperchromatism. These nuclear abnormalities fall short of those seen in PanIN-3. Mitoses are rare, but when present are non-luminal (not apical) and not atypical. True cribriforming luminal necrosis and marked cytologic abnormalities are generally not seen, and when present should suggest the diagnosis of PanIN-3.
High-grade
High-grade pancreatic intraepithelial neoplasia replaces the older term- PanIN-3.
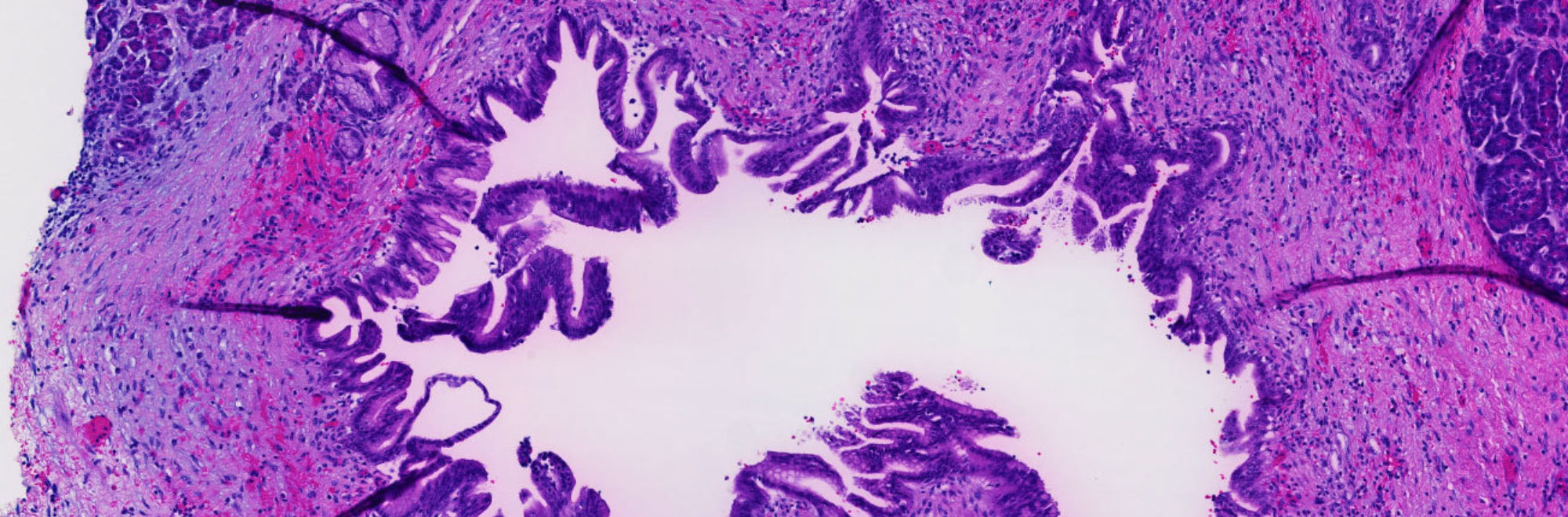
PanIN-3: (Pancreatic Intraepithelial Neoplasia 3): Architecturally, these lesions are usually papillary or micropapillary, however, they may rarely be flat. True cribriforming, budding off of small clusters of epithelial cells into the lumen and luminal necroses should all suggest the diagnosis of PanIN-3. Cytologically, these lesions are characterized by a loss of nuclear polarity, dystrophic goblet cells (goblet cells with nuclei oriented towards the lumen and mucinous cytoplasm oriented toward the basement membrane), mitoses which may occasionally be abnormal, nuclear irregularities and prominent (macro) nucleoli.
The Pathology Workshop participants noted that some ducts may have changes of more than one PanIN grade. In these instances, the lesion should be graded based on the highest grade component of a lesion.
Mimickers of PanIN
The Pathology Workshop participants noted that there are several mimickers of PanIN lesions that need to be recognized such as cancerization of ducts, intraductal papillary mucinous neoplasms (IPMN), and mucinous cystic neoplasms.
Reactive changes: Reactive changes may mimic PanINs. The presence of significant inflammatory cell infiltrates, particularly when there are numerous polymorphonuclear leukocytes, should raise the possibility of reactive changes.
Other Terms
A variety of older terms have been used to describe PanINs. These include:
| Term(s) | Definition |
|---|---|
| Squamous Metaplasia | Epidermoid metaplasia, multilayered metaplasia |
| PanIN-1A | Pyloric gland metaplasia, goblet cell metaplasia, mucinous hypertrophy, flat duct lesion without atypia, mucinous ductal hyperplasia, simple hyperplasia, mucinous cell hyperplasia, flat ductal hyperplasia, non-papillary epithelial hypertrophy. |
| PanIN-1B | Papillary hyperplasia, papillary duct lesion without atypia, and ductal hyperplasia. |
| PanIN-2 | Atypical hyperplasia, papillary duct lesion with atypia, low-grade dysplasia, and some cases of moderate dysplasia. Mucous metaplasia and pyloric gland metaplasia commonly involve small branch ducts or extend into lobules surrounding PanIN in ducts. Such involvement has been called adenomatoid or adenomatous hyperplasia, especially when the change dominates involvement of ductal epithelium. It is regarded as part of the spectrum of PanIN-1. |
| PanIN-3 | Carcinoma insitu, intraductal carcinoma, high-grade dysplasia, severe dysplasia, and some cases of moderate dysplasia. |
This nomenclature and these diagnostic criteria are meant to be a "working formulation," not a permanent final product. As was hoped, this nomenclature fostered the study of duct lesions. These studies included correlation of molecular genetic alterations with each grade of PanIN, the expression of antigens as determined immunohistochemically, correlation with cytologic findings and patient follow-up.
The long term goal is to detect and treat precancerous lesions before they become an invasive cancer.
Participants in the original think tank included:
| Participant | Affiliation at the time of the Think Tank |
|---|---|
| Ralph H. Hruban, M.D. | The Johns Hopkins Hospital |
| N. Volkan Adsay, M.D. | Harper Hospital & Wayne State Univ. |
| Jorge Albores-Saavedra, M.D. | Univ. of Texas, Southwestern |
| Carolyn Compton, M.D. | Massachusetts General Hospital |
| David Klimstra, M.D. | Memorial Sloan-Kettering Cancer Center |
| Gnter Klppel, M.D. | Univ. of Kiel |
| Daniel Longnecker, M.D. | Dartmouth-Hitchcock Medical Center |
| Jutte Lttges, M.D. | Univ. of Kiel |
| G. Johan Offerhaus, M.D., Ph.D. | Univ. of Amsterdam |
References
Hruban RH, Adsay NV, Albores-Saavedra J, Compton C, Garrett E, Goodman SN, Kern SE, Klimstra DS, Kloppel G, Longnecker DS, Luttges J, Offerhaus GJA. Pancreatic intraepithelial neoplasia (PanIN): A New nomenclature and classification system for pancreatic duct lesions. Am J Surg Pathol, 2001, volume 25:579-86
A revised classification system and recommendations from the Baltimore meeting for neoplastic precursor lesions in the pancreas. Basturk O, Hong SM, Wood LD, Adsay NV, Albores-Saavedra J, Biankin AV, Brosens LA, Fukushima N, Goggins M, Hruban RH, Kato Y, Klimstra DS, Klöppel G, Krasinskas A, Longnecker DS, Matthaei H, Offerhaus GJ, Shimizu M, Takaori K, Terris B, Yachida S, Esposito I, Furukawa T; Baltimore Consensus Meeting.Am J Surg Pathol. 2015 Dec;39(12):1730-41