

Pathology
Examination of a biopsy or the entire tumor under the microscope is the “gold standard” for establishing the diagnosis of a neuroendocrine tumor. Neuroendocrine tumors usually have a distinct microscopic appearance, and this appearance can be used to not only determine that the tumor is a neuroendocrine tumor, but also the specific type of neuroendocrine tumor. Special stains, called immunohistochemical stains, can be used to demonstrate the production of hormones, such as insulin and glucagon, in tissue sections made from biopsies or resected tumors. In addition to establishing a diagnosis, pathological examination can also help establish the prognosis, because prognosis for many neuroendocrine tumors is related to how fast the tumor is dividing and dividing cells can be seen and counted using a microscope.
Importance of Pathology
Although we often don’t think about them, pathologists make up a critical part of the team caring for patients with a neuroendocrine tumor. That is because the appearance of a neuroendocrine tumor under the microscope can provide important information on how the tumor should be treated.
The clinical behavior of neuroendocrine tumors is notoriously difficult to predict. Most are slow growing and some don’t even spread (metastasize). It turns out that subtle changes in how fast the tumor cells are dividing (reproducing) can make a big difference in how the tumors behave. Faster dividing tumors are more likely to spread than are slowly dividing tumors. For this reason, the accurate pathologic examination of neuroendocrine tumors is critical.
For example, in a landmark paper Dr. Trevor Ellison and the team at Johns Hopkins reported on 326 patients who had a neuroendocrine tumor of the pancreas surgically resected (Annals of Surgery 2013, PMID 23673766). They found that tumor grade, how fast the tumor cells are dividing, was the single most important prognostic indicator for these patients.
Here's how to get more information on having your pathology slides reviewed.
Blood Tests
Elevated levels of the hormones produced by neuroendocrine tumors can often be detected in the blood by special tests that can be run on blood samples taken from a patient. These tests are measured using immunoassays, including radioimmunoassay. Tests for chromogranin, insulin, gastrin, VIP, glucagon, somatostatin, pancreatic polypeptide, and other hormonal markers are typically performed at selected large medical center or reference laboratories.
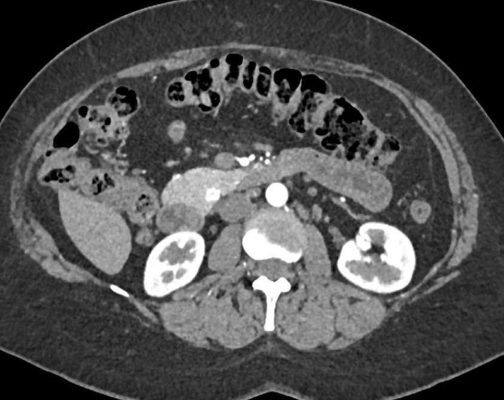
Localization and Staging
Computerized tomography (CT or CAT) remains one of the best imaging modalities for neuroendocrine tumors. The accuracy of the CT scan in tumor localization is improved by the use of contrast, and CT can be used to evaluate the patient for signs that the tumor has spread to lymph nodes or to distant organs. Neuroendocrine tumors often "enhance" in the arterial phase of a CT scan. This feature is believed to be a manifestation of the rich blood supply that these tumors have, and it is a helpful diagnostic feature.
Other tools for evaluating patients with a suspected neuroendocrine tumor include endoscopic ultrasound (EUS), magnetic resonance imaging (MRI) and angiography (visualizing the blood flow to the tumor with dye injected into the blood stream). The team at Johns Hopkins has reported that gastroenterologists can use EUS to help guide surgery by placing markers to indicate the location of small, difficult to visualize, tumors. Another technique that holds promise for the imaging of neuroendocrine tumors is "somatostatin receptor imaging." This technique takes advantage of the presence of somatostatin receptors on many neuroendocrine tumors. These scans are called "octreotide scans". Basically, a radioactive form of octreotide, a drug similar to somatostatin, is injected into the blood stream. It travels in the bloodstream and binds to (attaches to) neuroendocrine tumor cells that have the receptor for somatostatin on their surface. A radiation-measuring device can then detect the radioactive octreotide localized to the tumor.
In some rare instances very small neuroendocrine tumors cannot be visualized using standard imaging techniques and clinicians use intraventional radiology to selectively sample the blood in various parts of the body. These various samples can then be tested in the lab to see which one has the highest concentration of any hormones the tumor is making. The blood samples with the highest concentrations are likely to be those taken from closest to the tumor.